Sleep problems are common in Parkinson’s disease, but one often overlooked factor is how you sleep. Choosing the best sleep positions for Parkinson’s patients can help reduce stiffness, improve breathing, ease reflux, and make it easier to move in the morning. Rather than one “perfect” position, the goal is to match sleep posture to Parkinson’s-specific symptoms in a way that supports comfort, safety, and better rest.

Sleep problems are common in Parkinson’s disease, but one overlooked factor is sleep position. The “best” position is rarely one universal posture—because Parkinson’s symptoms (rigidity, tremor, pain, REM sleep behavior disorder, reflux, breathing problems, and blood pressure changes) vary widely. Still, research and clinical guidance point to a few positions that are consistently safer and more helpful for many people with Parkinson’s disease.
This guide explains the best sleep positions for Parkinson’s patients, who they help most, and how to set them up comfortably.
Why sleep position matters more in Parkinson’s disease
Many Parkinson’s patients spend more time sleeping on their back (supine) and may change position less overnight, partly due to nighttime slowness/rigidity. That matters because back-sleeping can worsen snoring and obstructive sleep apnea, while limited turning can increase discomfort and stiffness.
Position also interacts with common Parkinson’s-related issues like:
- Reflux or nighttime nausea
- Drooling/saliva pooling
- Shoulder/hip pain
- REM sleep behavior disorder (RBD) (dream enactment)
- Neurogenic orthostatic hypotension (blood pressure drop on standing)
So instead of asking “What is the best position?”, a better question is: Which position best supports your main problem at night?
1. Side sleeping (lateral) is the best “default” for many people
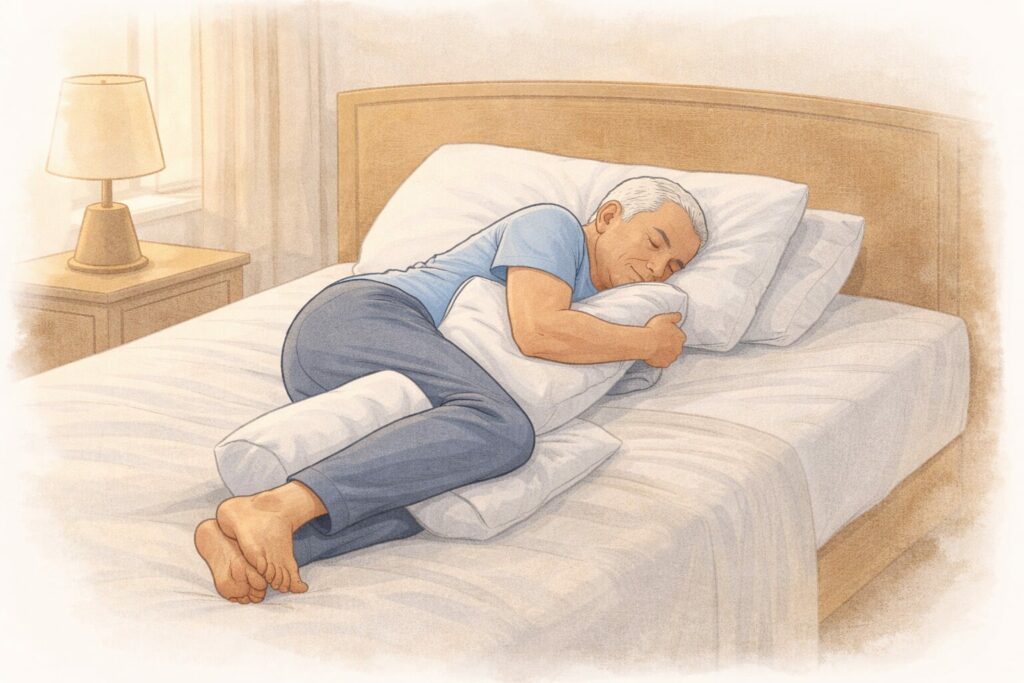
If you don’t have a special limitation (like severe shoulder pain on both sides), side sleeping is usually the best starting point for Parkinson’s patients.
Why it helps
- Breathing: Side sleeping often reduces airway collapse compared with sleeping flat on the back, which can matter because sleep apnea is common and back-sleeping can worsen it.
- Comfort: Many people find side sleeping reduces nighttime “locked” feeling versus lying flat, especially if turning is hard.
How to set it up (simple and effective)
- Put a pillow between the knees to reduce hip/back strain.
- Hug a small pillow to support the upper arm and reduce shoulder pulling.
- If you roll onto your back unintentionally, place a pillow behind your back to create a gentle “wedge” that discourages rolling.
Left side vs right side
If reflux is an issue, left-side sleeping has meaningful evidence: a systematic review and meta-analysis found left lateral decubitus sleep is associated with reduced nocturnal reflux and improved gastroesophageal reflux disease symptoms/quality of life.
This is especially relevant in Parkinson’s disease because reflux and slower stomach motility are common.
Practical takeaway: If reflux, sour taste, chronic cough at night, or heartburn is a problem, try left-side sleeping first.
Get Your Free Parkinson’s Medication Management Diary
Download your free printable diary to easily track your medications, symptoms, and doses.
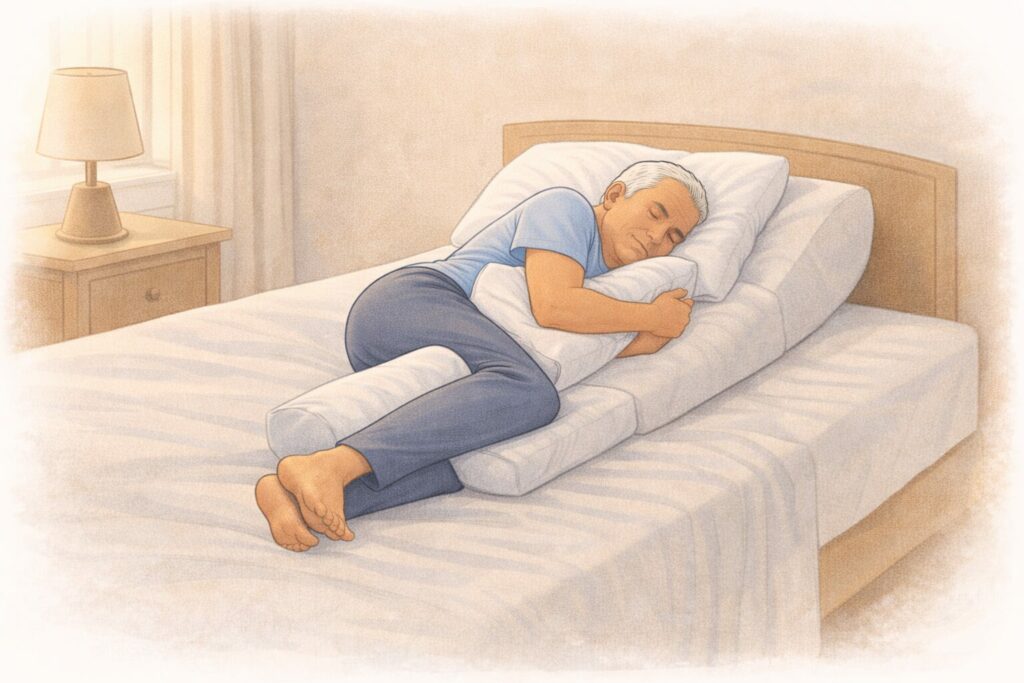
2) Slightly elevated back sleeping can be best for reflux, drooling, or morning blood pressure issues
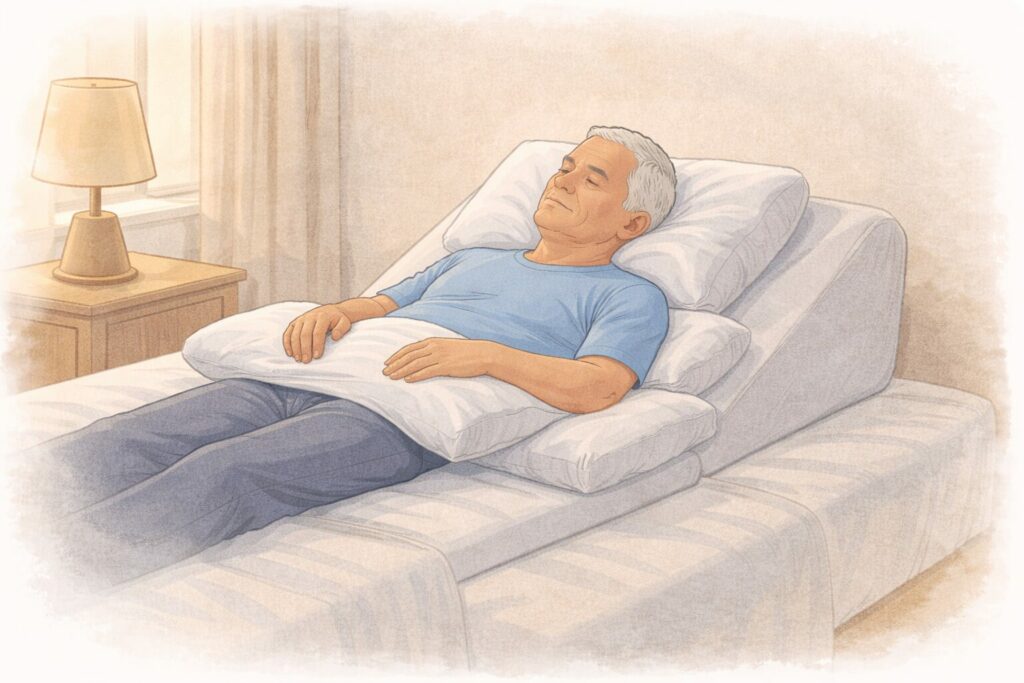
Some people simply cannot tolerate side sleeping (shoulder pain, severe hip pain, spinal issues). In that case, back sleeping can still be workable—if you modify it.
When it helps most:
- Nighttime reflux or regurgitation
- Drooling/saliva pooling
- Neurogenic orthostatic hypotension symptoms on rising (lightheadedness)
A neurology review on autonomic dysfunction in Parkinson’s disease notes that sleeping with the head of the bed elevated (around 30°) may reduce symptomatic Neurogenic orthostatic hypotension when standing up in the morning.
Head-of-bed elevation is also commonly recommended in aspiration-risk and reflux contexts.
How to do it safely (important)
- Prefer a wedge pillow or bed elevation under the mattress (more stable) rather than stacking multiple pillows (which can bend the neck).
- Aim for a gentle incline, not a steep “sit-up.”
Caution: If you have suspected or known obstructive sleep apnea, flat back sleeping can worsen breathing for many people. If you must sleep on your back, consider incline + discuss OSA evaluation with your clinician.
3) Avoid stomach sleeping (prone)

Stomach sleeping is rarely ideal in Parkinson’s disease.
Why it’s usually not recommended
- It can strain the neck and lower back
- It can make getting in/out of bed harder
- It may reduce chest expansion in some people
- It’s difficult to set up safely if you have stiffness, tremor, or mobility limits
If someone loves prone sleeping and feels best that way, it’s not automatically “forbidden”—but in Parkinson’s, it tends to be a high-effort position with more downside than benefit.
4) If you have REM Sleep Behavior Disorder (RBD), prioritize safety over “perfect posture”
RBD is common in Parkinson’s disease. The main goal isn’t a specific position—it’s preventing injury during dream enactment.
Clinical guidance from the Journal of Sleep Medicine emphasizes bed and partner safety strategies, including sleeping separately in severe cases and using barriers like pillows between partners.
Practical positioning ideas for RBD:
- Side sleeping can be fine, but focus on a safe bed setup:
- Remove sharp objects from the bedside
- Pad corners
- Consider placing the mattress low or using a floor mat beside the bed
- If episodes are intense, discuss treatment options with a sleep specialist (this is a medical issue, not just a “position” issue).
5) The “best position” depends on your main nighttime problem
Use this quick matching guide:
- Reflux/heartburn/nighttime cough: Left side first; or inclined back sleep.
- Suspected sleep apnea: Prefer side sleeping; ask about obstructive sleep apnea screening. Back-sleeping is commonly increased in Parkinson’s disease and is linked with sleep-disordered breathing concerns.
- Morning dizziness on standing: Consider head-of-bed elevation.
- Shoulder pain: Side sleep on the less painful side with pillow support; if both shoulders hurt, try an inclined back with arms supported by pillows.
- RBD (dream enactment): Safety setup first; position is secondary
Key takeaway
For many Parkinson’s patients, side sleeping (especially left side if reflux is an issue) is the best all-around position. If side sleeping isn’t possible, a gently inclined back position is often the next best option—particularly for reflux, drooling, or morning blood pressure symptoms. And if RBD is present, safety strategies matter more than any single posture.
Disclaimer: The information shared here should not be taken as medical advice. The opinions presented here are not intended to treat any health conditions. For your specific medical problem, consult with your healthcare provider.
Track your Parkinson’s day in less than a minute
The Parkinson’s Daily Diary App lets you record symptoms, medications, daily notes and doctor ready report in under a minute.